





Coronary bifurcation disease is present in up to 15–20 % of lesions undergoing percutaneous coronary intervention (PCI) and remains one of the outstanding challenges of treatment with PCI.1,2 PCI for coronary bifurcations is associated with more procedural complications and higher restenosis and adverse event rates than lesions in the body of the vessel.3–7 The introduction of drug-eluting stents (DES) for the treatment of bifurcation lesions has dramatically decreased restenosis rates from, in some subsets, up to 60 %8,9 to 5– 10 % and, in the latest trials,10–13 even to 2.5 % in the main branch, especially for patients suffering from diabetes.14 However, abrupt side branch closure and side branch ostial restenosis remain areas where further improvement is needed. A higher risk of subacute and late stent thrombosis is a major concern as well.7,10,15–18 Together with calcified lesions, saphenous vein grafts, chronic total occlusions and unprotected left main lesions, bifurcation lesions are complex lesions19 and therefore require a longer procedural time, more radiation exposure and higher volumes of contrast material in comparison with non-bifurcation lesions.20 This article explores several important questions about bifurcation lesions.
How Is a Bifurcation Lesion Defined and Which Classification Should be Used?
Many definitions of bifurcation lesions have been proposed, but the definition used by the European Bifurcation Club is that a bifurcation lesion presents as a coronary artery narrowing occurring adjacent to, and/or involving, the origin of a significant side branch. A significant side branch is a branch that you do not want to lose in the global context of a particular patient (symptoms, location of ischaemia, viability, collateralising vessel, left ventricular function, etc.)21 There are several major classifications of bifurcation lesions described in the literature,22–28 which are generally similar in describing specific bifurcation lesions and being sometimes difficult to memorise. The Medina classification is simple and practical; however, it does not include the description of angulation of branches and the size of the proximal healthy segment, as is the case in the classifications proposed by Movahed et al. and Shams et al. Nonetheless, the Medina classification has gained the highest popularity both in research and in clinical practice.29 Considering the increasing use and more objective analysis of bifurcation lesions with intravascular ultrasound (IVUS), a more specific and clinically relevant classification should be developed based on IVUS results.
Which Technique Should Be Used?
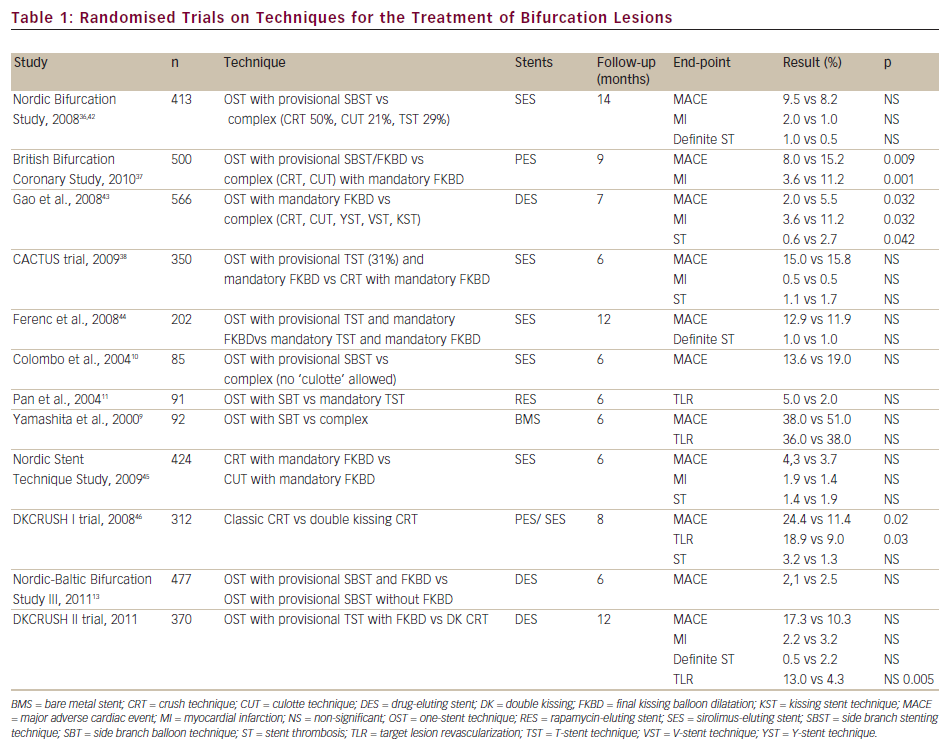
Coronary bifurcations are a unique and heterogeneous collection of anatomical variations. Different treatment strategies are employed based on plaque burden and the location and angulation of the bifurcated lesion. There have been many randomised studies (see Table 1) and analyses of non-randomised trials and registries30–33 published comparing different techniques and stents for the treatment of bifurcation lesions. Two meta-analyses of randomised controlled trials comparing a simple versus a complex strategy in the treatment of bifurcation lesions using DES revealed that a provisional strategy was associated with a reduction in myocardial infarction and a non-significant reduction in stent thrombosis rates.34,35 These data suggest that, although DES are preferable to bare-metal stents in bifurcation PCI, no additional benefit is associated with a mandatory two-stent strategy. At present, a one-stent technique – stenting the main branch with a DES and using a provisional side branch technique (side branch stenting or ballooning) – seems to be the prevailing approach.
Provisional stenting should be performed in bifurcation lesions with an intermediate-size side branch (diameter ≥2–2.75 mm), with stent deployment in the side branch only for suboptimal angiographic results, including flow-limiting dissection, residual stenosis >70 % or TIMI flow <2.36–38 Alternatively, when both the parent vessel and the side branch are large (≥2.5 to >2.75 mm), especially with significant disease distal to the ostium and when the side branch arises at a shallow angle, an elective two-stent approach might be more appropriate.19
The reverse T-stenting technique is the most commonly used provisional stenting strategy; however, this technique does not ensure complete coverage of the side branch.39,40 Since the side branch ostium is the most common site of angiographic restenosis, adequate coverage of this region is important.36 For this reason, the T-stenting technique should be considered in lesions that more closely resemble a true ‘T’ configuration with a side branch angulation over 70° to enable better coverage of the entire side branch.
When the side branch arises at a shallow angle, other two-stent techniques (crush, culotte or kissing stent) can be considered. Sharma et al. suggested an approach for choosing a two-stent technique on the basis of the size, angulation and obstruction of the side branch;41 however, the most important part of decision making is the operator’s experience.
Is Pre-dilation of the Side Branch Needed?
The best intervention for a bifurcation lesion is to stent the main branch without compromising any side branch. However, low-pressure balloon inflation of the side branch can help to prevent plaque shifting from the main branch lesion in high-risk situations. The advantage of this strategy is that the atherosclerotic material in the main branch is re-arranged to a large degree and further main branch stenting may not cause further plaque shifting; it will also help to avoid the need for subsequent side branch dilation through the side strut. One has to be aware of the potential for rupture of a plaque in the proximal part of the side branch, which would lead to the need for side branch stenting. To avoid this situation, it is important that balloon is not oversized and is inflated to a low pressure.
How Can Difficult Side Branch Access Be Solved?
The combination of plaque distribution and vessel anatomy determines scenarios in which side branch wiring requires great experience and technical skill. Successful difficult side branch access wiring can be achieved with use of an appropriate guidewire with an appropriately shaped tip curvature. A wide angle between the proximal main vessel and side branch together with marked side branch ostial disease make wiring especially challenging. A useful solution is to shape the tip with a wide smooth bend or with a double bend and to use a pullback wiring technique if antegrade technique does not work.
Another option is the Venture catheter (St Jude Medical, St Paul, MN, US), a deflectable-tip catheter system that offers a novel way to solve difficult side branch access. With this system, the guidewire may be directed towards the side branch after deflection of the catheter tip and then advanced in the side branch over the strong support of the catheter.47,48
In highly selected cases, when all other techniques have failed, a main vessel balloon pre-dilatation strategy can be used to wire the side branch. A typical situation is a bifurcation with a large plaque burden in both the main vessel and side branch and a wide take-off angle. This technique is not advisable as it may cause plaque and carina shift, ultimately resulting in side branch occlusion. In the optimal scenario, gentle pre-dilatation of the proximal main vessel may create enough space in the main vessel and change the angle for successful advancement of a bent wire towards the side branch. In some cases, debunking techniques such as rotational atherectomy or a scoring device can be used as a pre-dilatation tool.
How Should Unfavourable Side Branch Anatomy Be Re-wired After Main Vessel Stent Placement?
Difficult access to the side branch or main branch can occur either at the start of the procedure or after side branch or main branch stenting. Difficulty may occur when re-crossing the stent struts with a guidewire or advancing a balloon through the stent struts, especially with three layers of struts if the crush technique is used. In recent years it has been recognised that crossing the distal side cells of the main vessel stent is associated with better ostium scaffolding and reduced need for side branch stenting.23,49 Re-wiring into very distal part of the side branch ostium can be achieved using the pullback re-wiring technique. Although re-wiring does not represent a problem in the majority of bifurcated lesions, there are some procedures that are highly technically demanding. Longer tips and wide curves are often required in the case of occluded side branches. Sometimes, difficulties with re-wiring are associated with under-expanded stent struts in the main vessel, prohibitive angulation of side branch take-off or the presence of proximal vessel tortuosities. In the case of compromised flow in an important side branch and failure after multiple re-wiring attempts, a 1.5 mm over-the-wire balloon or an open-end catheter can be advanced near the origin of the side branch to increase the support of the wire crossing the struts; alternatively, a ‘rescue’ jailed balloon technique can be applied by using the wire jailed in the side branch to advance a small balloon at the side branch ostium under the main vessel stent.
Is Side-strut Dilation Beneficial?
It has been demonstrated that side branch dilation through a stent consistently results in narrowing of the main stent lumen immediately downstream from the side branch; this narrowing increases in severity with increasing size and inflation pressure of the balloon used for side branch dilation. Redilation of the main branch stent lumen alone then results in some reduction in the size of the side branch lumen. This problem can best be avoided by ending the procedure with kissing balloon dilation of both the main branch and the side branch as this helps restore main branch geometry and expansion.50,51
Complications of Bifurcation Lesion Stenting
Side Branch Closure
Side branch closure is reported in 4.5–26 % of cases using a one-stent technique for bifurcation lesions and is mainly attributable to plaque shifting, side branch ostial recoil and/or propagation of dissection. Anatomical features associated with increased risk of side branch closure include side branch size (small side branch reference diameter,)52 steep angulation from the main vessel,53 side branch ostial involvement and side branch ostial composition. Acute coronary syndrome has also been reported as a predictive factor of abrupt side branch closure.1 Stent-induced occlusion of a large side branch may result in significant myocardial ischaemia and infarction, although in most patients the long-term prognosis is excellent and most initially occluded side branches are patent at late angiographic follow-up.53,54
When the side branch ostium is not diseased, the likelihood of its narrowing after the main vessel is stented is low, and the side branch can be rescued by kissing balloon inflation of the main vessel stent and side branch if it is compromised. A challenging situation is a significant true bifurcation lesion with atherosclerotic involvement of both the main vessel and side branch ostia. Provisional T-stenting is associated with a higher risk of side branch occlusion.
In the randomised trial published by Baim et al., atherosclerotic involvement of both branch ostia was associated with a 40 % occurrence of myocardial infarction. However, if the side branch was not involved, myocardial infarction occurred in only 4.7 %.55 In an analysis of angiographic predictors of side branch occlusion, side branch closure occurred in 65 % of lesions if both ostia were diseased compared with 4 % in lesions without side branch involvement.53 The Nordic study36 showed that the presence of over 50 % of lesions in the side branch was associated with a restenosis rate of 11–19 %, whereas less than 50 % side branch disease was associated with an in-stent restenosis rate of 4.6–5 %.
Based on these trials, if a bifurcation lesion does not have high-risk features for side branch occlusion, such as involvement of both branch ostia or steep angulations, using a one-stent technique – or the side branch technique with provisional side branch stenting in the case of unsatisfactory results in the side branch – is the preferred technique. Otherwise, two-stent techniques offer safer access to both diseased branches in high-risk lesions.56 Revascularisation of side branch vessels with a diameter under 1.5 mm is unlikely to yield any benefits; therefore, vessels of this size are routinely excluded from studies comparing bifurcation stenting strategies.36,38 Conversely, in large side branch vessels (diameter over 2.75 mm) with significant disease distal to the ostium, an elective two-stent approach might be more appropriate.19
Side Branch Restenosis
Major clinical, angiographic and IVUS risk factors for restenosis have been identified: small reference vessel diameter, small minimal stent area, long lesion (or stent) and diabetes mellitus.57–59 In the DES era, in-stent restenosis reduction in the main branch from up to 40–60 % to 2.5 % has been achieved in certain subsets of patients; however, restenosis at the ostium of the side branch remains a stubborn problem60 and cause for repeated revascularisations. The probable mechanisms could be focal stent underexpansion at the ostium, inadequate ostial scaffolding or uneven drug distribution.61
Stent Thrombosis
Pathological studies have suggested that arterial branch points are the foci of low shear stress and low flow velocity and are sites predisposed to the development of atherosclerotic plaque, thrombus and inflammation. The two or three layers of stent struts (with the crush technique) apposed to the vessel wall initially raised concerns about possible increased thrombogenicity especially with DES.
Stent thrombosis is present in up to 4.4 % of patients after PCI of bifurcation lesions compared with around 1.4 % of patients with non-bifurcation lesions.6 The risk of subacute stent thrombosis has been higher using two-stent techniques in the majority of trials.10,30,32 Moreover, stent thrombosis rates appear to be approximately doubled when two DES rather than one are implanted in a bifurcation.10,17 Treatment of bifurcations has been identified as an independent predictor of late stent thrombosis.62
Fracture of a Jailed Wire
Hydrophilic guidewires should be used cautiously both for wire jailing and when re-crossing into the side branch owing to the risk of stripping the polymer coating wire when withdrawing and the risk of wire-induced dissection or perforation. When the jailed wire technique is used, the stent in the main vessel should be implanted with low atmospheres; re-wiring should then be performed and only then should postulation at a higher atmosphere be undertaken.50 Also, jailing a long segment of wire in the parent vessel should be avoided.
Jailed wire fracture is a rare but serious complication of percutaneous coronary bifurcation interventions. Therefore, insertion of a wire into the side branch must be significantly considered even though the jailed wire technique is preferred by most operators. Moreover, the side branch must be re-wired by a second wire and the jailed wire removed after main branch stenting at a low atmosphere; only then should post-dilatation stenting at a high atmosphere be performed. Rupture of the jailed wire is described in the literature;1 however, brief descriptions of successful interventional management of complications are lacking. Removal of a broken wire is very difficult or even impossible because power is needed to pull the wire, especially if high atmospheres were used for stent implantation.
The technique of snaring with a loop-snare device could be the method of choice when a jailed wire is broken and the free proximal filament is located in the guiding catheter or proximally in the main branch. Before pulling the system out, a harder guidewire should be introduced under the stent struts into the diagonal branch and a small balloon should be used to dilate the space between the vessel wall and the stent struts. In the literature, successful retrieval of fragments of devices and catheters using the snaring device technique have been described, but not of a jailed wire.63
Another method of choice in the case of a jailed, broken wire is inflation of a balloon with 20 atmospheres in the guiding catheter. The inflated balloon will press the free part of the filament in the guiding catheter, allowing removal of the whole system together with the guiding catheter from the coronary artery. However, this method carries some risks and may be ineffective, and is mainly applicable in cases where a free, proximal filament of the jailed wire is in the guiding catheter.
If the interventions described above are not possible or successful, or if a free filament of broken wire is located in the coronary artery and the wire is broken proximally to the floppy part, surgery is required urgently.64
Dedicated Bifurcation Stents
The less favourable outcomes associated with bifurcation compared with non-bifurcation lesions may in part result from the inability of current devices and techniques to scaffold adequately and preserve the side branch ostium, which is the common site of restenosis. The main requirement of a stent dedicated to bifurcation lesions is the ability to stent bifurcations using a straightforward technique reliably, achieving complete lesion coverage and scaffolding.65
Intravenous Ultrasound in Bifurcation Stenting
IVUS should be considered in the assessment of patients with coronary bifurcation lesions, particularly in those with angiographically ambiguous left main coronary artery disease. Better insight into plaque configuration using IVUS can diminish the unnecessary use of the two-stent procedure by distinguishing ‘true stenosis’ from ‘pseudostenosis’ caused by artefacts, including coronary spasm or calcification at the side branch. This knowledge may allow better selection of the most appropriate stenting technique and reduce the need for a two-stent strategy. Moreover, IVUS may reduce the long-term mortality rate of PCI, especially when DES are used for unprotected left main stenosis.66,67
Conclusions
Coronary bifurcation disease remains one of the outstanding challenges of treatment with PCI, especially in complex situations as very calcified true bifurcation lesions with steep angulation or long side branch lesions. Many unpredictable difficult situations and complications can occur which require great experience and technical skill on the part of the operator. Special bifurcation-dedicated stents have been developed and are under investigation to stent bifurcations using a straightforward and reliable technique to achieve complete lesion coverage and scaffolding. IVUS should be considered in the assessment of patients with coronary bifurcation lesions.